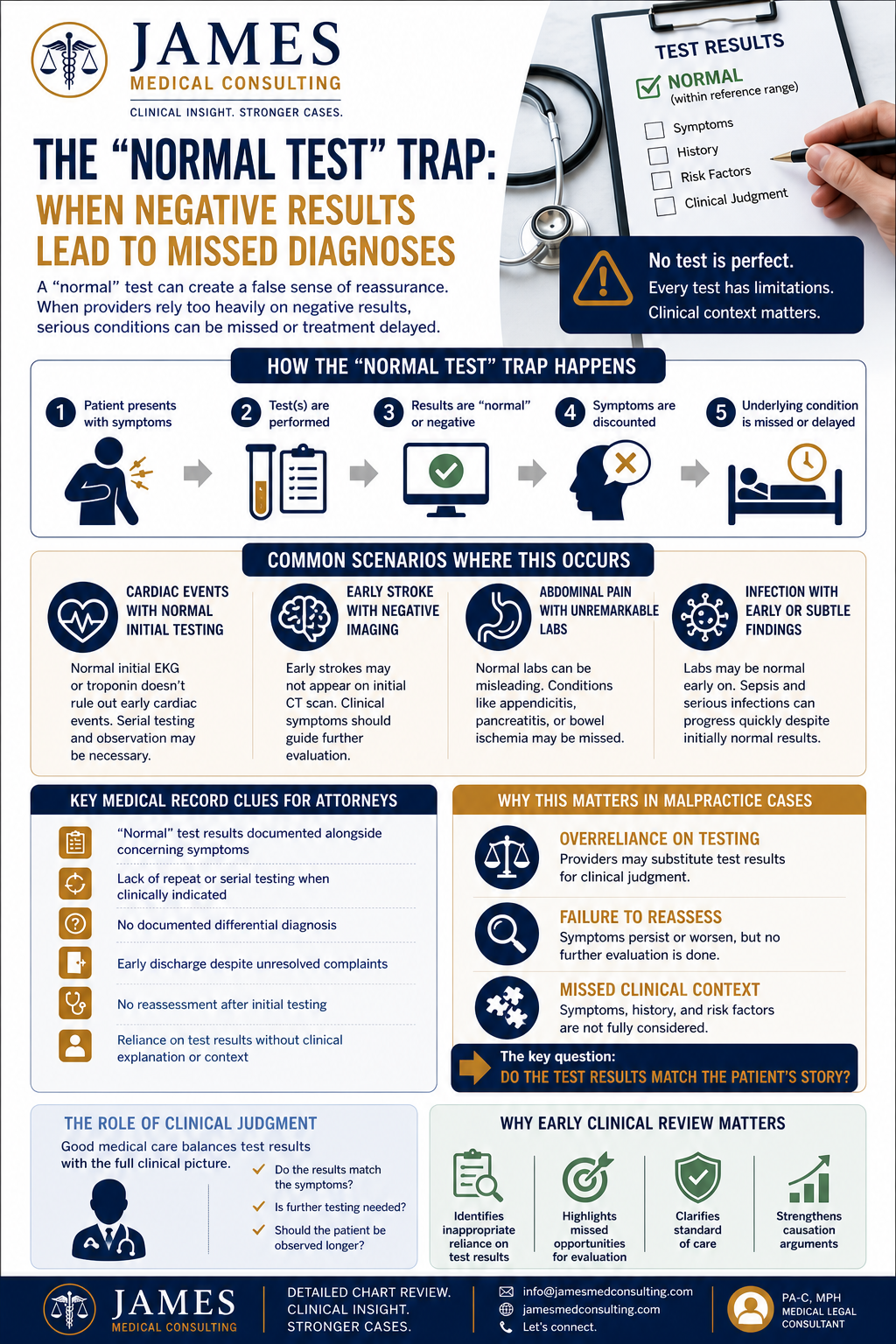
The “Normal Test” Trap: When Negative Results Lead to Missed Diagnoses
Introduction
In medical malpractice cases, abnormal results often get the most attention.
But sometimes, the real issue isn’t what was abnormal—it’s what was labeled “normal.”
A “normal” test result can create a false sense of reassurance. When providers rely too heavily on a single negative test, it can lead to missed diagnoses, delayed treatment, and significant patient harm.
For attorneys, these cases often hinge on one critical question:
Was the negative test result interpreted appropriately within the full clinical picture?
What Is the “Normal Test” Trap?
The “normal test” trap occurs when:
A provider relies on a negative test result
Symptoms are discounted because of that result
Further evaluation is not pursued
The underlying condition is missed or delayed
In reality, no test is perfect. Every diagnostic tool has limitations, sensitivity thresholds, and clinical context requirements.
Common Scenarios Where This Occurs
1. Cardiac Events with Normal Initial Testing
Example:
A patient presents with chest pain but has a normal initial EKG or troponin.
Issue:
Early cardiac events may not be immediately detectable.
Serial testing and observation are often required.
2. Early Stroke with Negative Imaging
Example:
A CT scan is read as normal despite neurological symptoms.
Issue:
Early strokes may not appear on initial imaging.
Clinical symptoms should guide further evaluation.
3. Abdominal Pain with Unremarkable Labs
Example:
Normal labs lead to discharge, but the patient later returns with appendicitis or another surgical condition.
4. Infection with Early or Subtle Findings
Example:
Normal white blood cell count despite early sepsis.
Issue:
Lab values may lag behind clinical deterioration.
Why This Matters in Malpractice Cases
These cases are powerful because they often involve:
Overreliance on Testing
Providers may substitute test results for clinical judgment.
Failure to Reassess
Patients are not reevaluated when symptoms persist or worsen.
Missed Clinical Context
Symptoms, history, and risk factors are not fully considered.
Key Medical Record Clues for Attorneys
When reviewing records, look for:
“Normal” test results documented alongside concerning symptoms
Lack of repeat or serial testing when clinically indicated
No documented differential diagnosis
Early discharge despite unresolved complaints
No reassessment after initial testing
Documentation that relies heavily on test results without clinical explanation
These patterns often reveal gaps in care.
The Role of Clinical Judgment
Good medical care requires balancing test results with clinical evaluation.
Providers should ask:
Does the test result match the patient’s symptoms?
Is further testing needed?
Should the patient be observed longer?
When this doesn’t happen, errors can occur.
Why Early Clinical Review Matters
“Normal test” cases can be subtle but highly significant.
Early review can:
Identify inappropriate reliance on test results
Highlight missed opportunities for further evaluation
Clarify whether the standard of care was met
Strengthen causation arguments
How I Help Attorneys Identify These Issues
Through detailed chart review, I help attorneys:
Analyze test results in the context of symptoms
Identify gaps in clinical reasoning
Highlight failures in reassessment or follow-up
Translate medical data into clear legal insights
Conclusion
A normal test result doesn’t always mean everything is normal.
In fact, it can sometimes be the very thing that leads to a missed diagnosis.
For attorneys, understanding the limitations of diagnostic testing—and how it should be applied—can uncover powerful opportunities within a case.
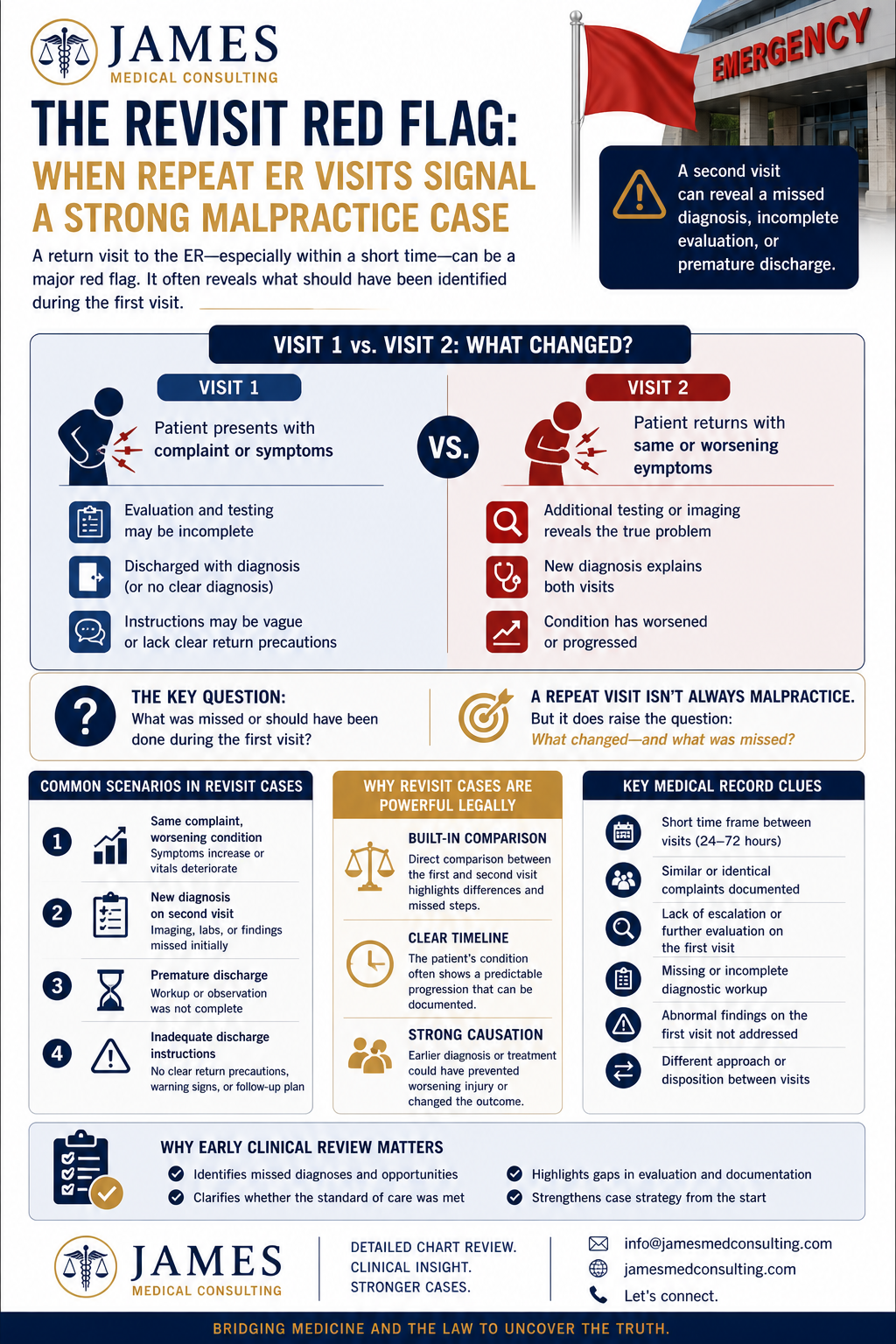
The Revisit Red Flag: When Repeat ER Visits Signal a Strong Malpractice Case
Introduction
In emergency medicine, patients sometimes return.
But when a patient comes back to the emergency department with the same complaint—especially within a short time frame—it can be a major red flag.
For attorneys, repeat visits often point to something deeper:
A missed diagnosis, incomplete evaluation, or premature discharge.
As a Physician Assistant reviewing charts, I frequently see revisit cases where the second visit reveals what should have been identified the first time.
Why Repeat Visits Matter
A return visit isn’t automatically malpractice.
But it raises an important question:
What changed—and what was missed?
In many cases, the condition didn’t suddenly appear.
It was already developing during the initial visit.
Common Scenarios in Revisit Cases
1. Same Complaint, Worsening Condition
The patient returns with:
Increased pain
New or worsening symptoms
Deteriorating vital signs
Example:
A patient presents with abdominal pain, is discharged, and returns with appendicitis or a surgical emergency.
2. New Diagnosis on Second Visit
The second visit often leads to:
Imaging that wasn’t ordered initially
Lab abnormalities that were missed
A diagnosis that explains both visits
Red Flag:
Why wasn’t this identified the first time?
3. Premature Discharge
Patients may be discharged before:
Adequate observation
Complete workup
Symptoms are properly evaluated
4. Inadequate Discharge Instructions
Patients may not be given:
Clear return precautions
Specific warning signs
Follow-up instructions
This can delay appropriate care.
Key Medical Record Clues
When reviewing revisit cases, look for:
Short time frame between visits (24–72 hours is especially important)
Similar or identical complaints documented
Lack of escalation during the first visit
Missing or incomplete diagnostic workup
Abnormal findings on the first visit that were not addressed
Differences in provider approach between visits
These patterns often reveal missed opportunities.
Why Revisit Cases Are Powerful Legally
Revisit cases often provide:
A Built-In Comparison
Attorneys can directly compare:
First visit vs. second visit
What was done vs. what should have been done
Clear Timeline of Progression
The patient’s condition often shows a predictable progression.
Strong Causation Arguments
If earlier diagnosis or treatment could have changed the outcome, causation becomes clearer.
The Role of Documentation
Documentation from both visits is critical.
Pay attention to:
Vital signs and trends
Provider notes and decision-making
Discharge instructions
Diagnostic testing differences
Inconsistencies between visits can be key.
Why Early Clinical Review Matters
Revisit cases can quickly reveal whether a case has merit.
Early review can:
Identify missed diagnoses
Highlight inadequate initial evaluation
Clarify whether the standard of care was met
Strengthen case strategy early
How I Help Attorneys Analyze Revisit Cases
Through detailed chart review, I help attorneys:
Compare first and second visit documentation
Identify missed opportunities during the initial encounter
Analyze progression of symptoms and findings
Translate clinical timelines into clear legal insights
Conclusion
A repeat visit is more than just a second encounter—it’s a second chance.
And when that second chance reveals what should have been caught the first time, it can become a powerful foundation for a malpractice case.
For attorneys, recognizing the significance of revisit patterns can uncover opportunities that might otherwise be missed.
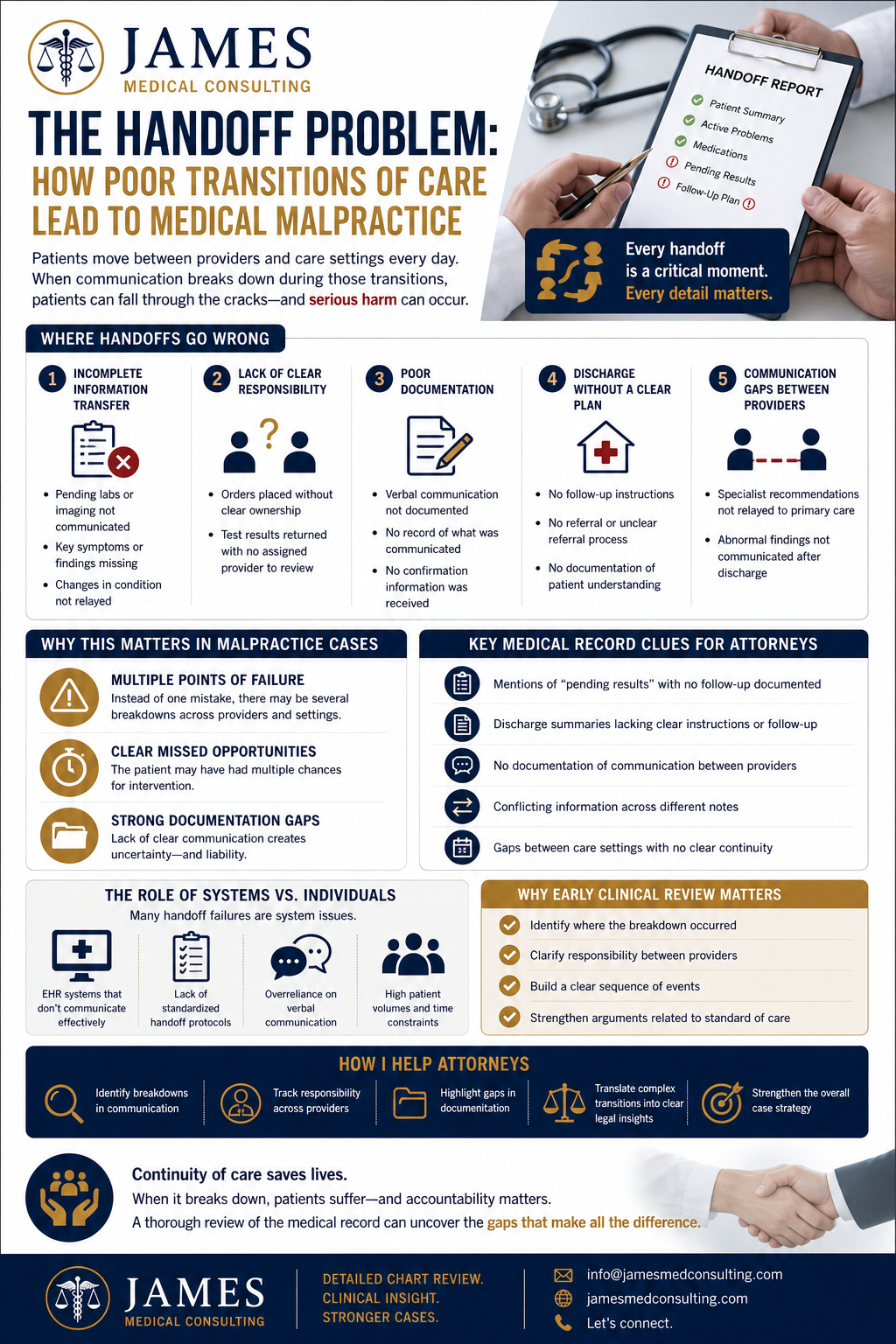
The Handoff Problem: How Poor Transitions of Care Lead to Medical Malpractice
Introduction
In healthcare, patient care is rarely handled by just one provider.
Patients move between emergency departments, hospital teams, specialists, and outpatient providers. And every time that happens, there’s a critical moment where information must be accurately transferred.
That moment is called a handoff—and when it breaks down, the consequences can be serious.
For attorneys, poor transitions of care are a common—and often overlooked—source of medical malpractice liability.
What Is a “Handoff”?
A handoff (or transition of care) occurs anytime responsibility for a patient is transferred from one provider or setting to another.
Common examples include:
Emergency department to inpatient admission
Shift changes between providers
Hospital discharge to primary care
Referral to a specialist
Each handoff requires clear, accurate, and complete communication.
Where Handoffs Go Wrong
1. Incomplete Information Transfer
Critical details may be missing during transitions.
Examples:
Pending lab or imaging results not communicated
Key symptoms or findings not documented
Changes in patient condition not relayed
2. Lack of Clear Responsibility
It’s not always clear who is responsible for follow-up.
Red Flag:
Orders placed without clear ownership
Test results returned with no assigned provider to review
3. Poor Documentation
Handoff communication is often verbal—and not fully documented.
Issue:
No record of what was communicated
No confirmation that information was received
4. Discharge Without a Clear Plan
Hospital and ED discharges are high-risk points.
Common Problems:
No follow-up instructions
No referral or unclear referral process
No documentation of patient understanding
5. Communication Gaps Between Providers
Different providers may operate in separate systems or workflows.
Examples:
Specialist recommendations not relayed to primary care
Abnormal findings not communicated after discharge
Why This Matters in Malpractice Cases
Handoff failures are powerful in litigation because they often involve:
Multiple Points of Failure
Instead of one mistake, there may be several breakdowns across providers.
Clear Missed Opportunities
The patient may have had multiple chances for intervention.
Strong Documentation Gaps
Lack of clear communication creates uncertainty—and liability.
Key Medical Record Clues for Attorneys
When reviewing records, look for:
Mentions of “pending results” with no follow-up
Discharge summaries lacking clear instructions
No documentation of communication between providers
Conflicting information across different notes
Gaps between care settings with no clear continuity
These patterns often indicate a breakdown in the transition of care.
The Role of Systems vs. Individuals
Many handoff failures are not just individual mistakes—they are system issues:
EHR systems that don’t communicate effectively
Lack of standardized handoff protocols
Overreliance on verbal communication
High patient volumes and time constraints
Understanding this can help frame the case more effectively.
Why Early Clinical Review Matters
Handoff-related cases can be complex, involving multiple providers and timelines.
Early review can:
Identify where the breakdown occurred
Clarify responsibility between providers
Build a clear sequence of events
Strengthen arguments related to standard of care
How I Help Attorneys Analyze Handoff Failures
Through detailed chart review, I help attorneys:
Identify breakdowns in communication
Track responsibility across providers
Highlight gaps in documentation
Translate complex transitions into clear legal insights
Conclusion
In healthcare, continuity of care is critical.
When that continuity breaks down, patients can fall through the cracks—and that’s where malpractice cases often begin.
For attorneys, recognizing failures in handoffs can uncover powerful opportunities within the medical record.

The “Stable” Patient Myth: When Normal Vital Signs Hide Serious Medical Errors
Introduction
In medical records, the word “stable” appears everywhere.
But in medical malpractice cases, that single word can be misleading—and sometimes dangerously inaccurate.
For attorneys reviewing cases, one of the most important questions to ask is:
Was the patient truly stable… or just documented that way?
As a Physician Assistant reviewing charts, I frequently see cases where documentation suggests stability, while the underlying data tells a very different story.
What Does “Stable” Actually Mean?
Clinically, “stable” should indicate that a patient’s condition is:
Not deteriorating
Hemodynamically sound
Not in immediate danger
However, in practice, the term is often used loosely or inaccurately—sometimes without proper clinical support.
Where the Problem Begins
1. Inconsistent Vital Signs
Vital signs are one of the most objective indicators of patient status.
Red Flags:
Tachycardia (elevated heart rate)
Hypotension (low blood pressure)
Fever or hypothermia
Abnormal respiratory rates
Issue:
Notes may state “patient stable” despite clearly abnormal vitals.
2. Lack of Trending
A single “normal” vital sign doesn’t tell the whole story.
What’s often missed:
Worsening trends over time
Fluctuating vital signs without reassessment
Lack of serial monitoring in high-risk patients
3. Copy-and-Paste Documentation
“Stable” is frequently carried forward in templated notes.
Red Flag:
Multiple entries stating “stable” without updated clinical evaluation
This can create a false narrative in the chart.
4. High-Risk Complaints Labeled as Stable
Certain symptoms should never be casually labeled as stable without thorough evaluation:
Chest pain
Shortness of breath
Abdominal pain
Neurological symptoms
Issue:
Premature labeling can lead to missed or delayed diagnoses.
Why This Matters in Malpractice Cases
The term “stable” can significantly impact how a case is interpreted.
Credibility Issues
If documentation says “stable” but vitals and findings suggest otherwise, it undermines provider credibility.
Missed Escalation
Patients who are incorrectly labeled as stable may not receive:
Additional testing
Specialist consultation
Appropriate monitoring
Causation
Failure to recognize instability can delay treatment—and worsen outcomes.
Key Medical Record Clues for Attorneys
When reviewing charts, look for:
The word “stable” used despite abnormal vital signs
Lack of documented reassessments
Missing trends in vital signs over time
Contradictions between objective data and provider notes
Early discharge in patients with unresolved abnormal findings
These inconsistencies often reveal deeper issues in care.
The Role of Nursing Documentation
Nursing notes can provide critical insight.
Often, they document:
More frequent vital signs
Changes in patient condition
Symptoms not reflected in provider notes
Comparing nursing and provider documentation can uncover important discrepancies.
Why Early Clinical Review Matters
Cases involving “stable” documentation often require careful interpretation of clinical data.
Early review can:
Identify inconsistencies between documentation and actual findings
Clarify whether the patient met criteria for stability
Highlight missed opportunities for intervention
Strengthen arguments related to standard of care and causation
How I Help Attorneys Identify These Issues
Through detailed chart review, I help attorneys:
Analyze vital sign trends and clinical data
Identify discrepancies in documentation
Highlight inappropriate use of terms like “stable”
Translate medical findings into clear legal insights
Conclusion
In medical malpractice cases, words matter.
And few words are more commonly misunderstood—or misused—than “stable.”
For attorneys, looking beyond the label and focusing on the data can uncover critical insights that shape the strength of a case.

Informed Consent Failures: A Hidden Weak Point in Medical Malpractice Cases
Introduction
In medical malpractice litigation, much of the focus is placed on diagnosis and treatment decisions. But in many cases, liability stems from something less obvious—and often overlooked:
Failure to obtain proper informed consent.
Even when a procedure is performed correctly, a lack of adequate patient understanding can create significant legal exposure. For attorneys, informed consent issues can open an entirely different pathway to establishing negligence.
What Is Informed Consent?
Informed consent is more than just a signed form.
It is a process of communication between the provider and the patient that includes:
The nature of the procedure or treatment
The risks and potential complications
Reasonable alternatives
The option to decline treatment
The key element is understanding—not just documentation.
Where Informed Consent Breaks Down
1. Generic or Template Consent Forms
Many facilities rely on standardized forms that lack patient-specific details.
Red Flag:
Broad language like “risks explained” with no specifics
Legal Impact:
Weakens the argument that the patient truly understood the risks.
2. Lack of Documented Discussion
The consent form may be signed—but there is no documentation of the actual conversation.
What’s Missing:
No note describing risks discussed
No mention of alternatives
No indication of patient questions
3. High-Risk Procedures Without Detailed Consent
Certain procedures require a higher level of explanation.
Examples:
Surgical interventions
Invasive diagnostic procedures
High-risk medications
If complications occur, lack of detailed consent becomes a major issue.
4. Language Barriers and Health Literacy
Consent is not valid if the patient does not fully understand.
Red Flags:
No interpreter documented for non-English-speaking patients
Complex medical terms without explanation
No confirmation of patient understanding
5. Timing of Consent
Consent obtained under pressure or too close to the procedure can be challenged.
Example:
Consent signed immediately before surgery without adequate time for consideration
Why This Matters in Malpractice Cases
Informed consent cases are unique because they focus on patient autonomy, not just clinical decision-making.
Attorneys can argue:
The patient would have declined the procedure if properly informed
The risk that occurred was not adequately disclosed
The provider failed to meet the communication standard of care
This can create liability even when the procedure itself was technically appropriate.
Key Medical Record Clues to Look For
When reviewing charts, look for:
Signed consent forms with vague or generic language
No accompanying provider documentation of discussion
Missing notes about risks, benefits, or alternatives
Lack of interpreter services documentation
Consent obtained immediately prior to procedure
Discrepancies between documented risks and actual complications
These details can significantly strengthen a case.
The Role of Documentation in Consent
Just like clinical care, if it’s not documented, it didn’t happen—at least from a legal standpoint.
Strong documentation should include:
Specific risks discussed
Alternatives presented
Patient questions and responses
Confirmation of understanding
Without this, the defense becomes much harder.
Why Early Clinical Review Matters
Informed consent issues are often subtle and easily overlooked.
Early case review can:
Identify gaps in the consent process
Clarify whether documentation meets the standard of care
Strengthen arguments related to patient understanding
Provide a clearer strategy for litigation
How I Help Attorneys Evaluate Consent Issues
Through detailed chart review, I help attorneys:
Identify deficiencies in the consent process
Analyze whether risks were appropriately communicated
Highlight documentation gaps
Translate medical records into clear legal insights
Conclusion
Informed consent is not just a form—it’s a process.
And when that process breaks down, it can create significant legal exposure, even in otherwise well-managed cases.
For attorneys, recognizing these gaps can uncover opportunities that might otherwise go unnoticed.

Delayed Diagnosis: How Timing Can Define a Medical Malpractice Case
Introduction
In medical malpractice litigation, it’s not always about whether a diagnosis was made—it’s about when it was made.
A delayed diagnosis can be just as harmful as a missed one. In many cases, the condition was eventually identified, but the delay in recognition or treatment led to a worse outcome.
For attorneys, these cases often hinge on one critical question:
Would earlier intervention have changed the outcome?
What Is a Delayed Diagnosis?
A delayed diagnosis occurs when:
Symptoms are present but not appropriately evaluated
Diagnostic testing is postponed or not ordered
Abnormal findings are not acted on in a timely manner
A condition is identified only after it has progressed
Unlike a complete failure to diagnose, these cases involve missed opportunities over time.
Common Conditions Involved in Delayed Diagnosis Cases
Certain conditions are more frequently associated with delays:
1. Stroke
Early recognition is critical.
Red Flag:
Neurological symptoms documented without appropriate imaging or stroke workup
2. Sepsis
Often subtle early on—but rapidly progressive.
Red Flag:
Abnormal vital signs (fever, tachycardia) without escalation or reassessment
3. Cancer
Delays often occur in follow-up of abnormal imaging or labs.
Red Flag:
Suspicious findings noted but not communicated or pursued
4. Cardiac Events
Chest pain cases are high risk.
Red Flag:
Incomplete cardiac workup or premature discharge
Where Delays Typically Occur
Emergency Departments
Failure to recognize evolving symptoms
Early discharge before full evaluation
Primary Care
Failure to act on abnormal labs or imaging
Delayed referrals to specialists
Transitions of Care
Poor communication between providers
Follow-up plans not clearly documented
Key Medical Record Clues
When reviewing charts, look for:
Timeline gaps between symptom onset and diagnosis
Abnormal findings that were not immediately addressed
Lack of escalation despite worsening condition
Repeated visits for the same complaint without resolution
Delayed ordering of appropriate diagnostic tests
These details help establish where the delay occurred—and why it matters.
Why Timing Is Critical Legally
Delayed diagnosis cases often provide a clear framework for causation:
What was known and when
What should have been done at that time
How the delay changed the patient’s outcome
In many cases, earlier diagnosis could have:
Prevented progression
Reduced severity of harm
Improved survival or recovery
This makes timing a powerful factor in litigation.
The Role of Documentation
Documentation is essential in establishing the timeline.
Key elements include:
Time-stamped vital signs and assessments
Provider notes across multiple visits
Diagnostic test results and when they were reviewed
Discharge instructions and follow-up plans
When the timeline doesn’t align with the patient’s condition, it raises serious questions.
Why Early Case Review Matters
Delayed diagnosis cases require careful analysis of progression over time.
Early clinical review can:
Build a clear timeline of events
Identify missed opportunities for intervention
Clarify whether the standard of care was met
Strengthen causation arguments
How I Help Attorneys Analyze Delayed Diagnosis Cases
Through detailed chart review, I help attorneys:
Reconstruct timelines from complex medical records
Identify where delays occurred
Highlight deviations from the standard of care
Translate clinical progression into clear legal insights
Conclusion
In medical malpractice cases, timing can be everything.
A diagnosis made too late can have the same—or greater—impact as one never made at all.
For attorneys, understanding where delays occurred and how they affected the outcome is key to building a strong case.
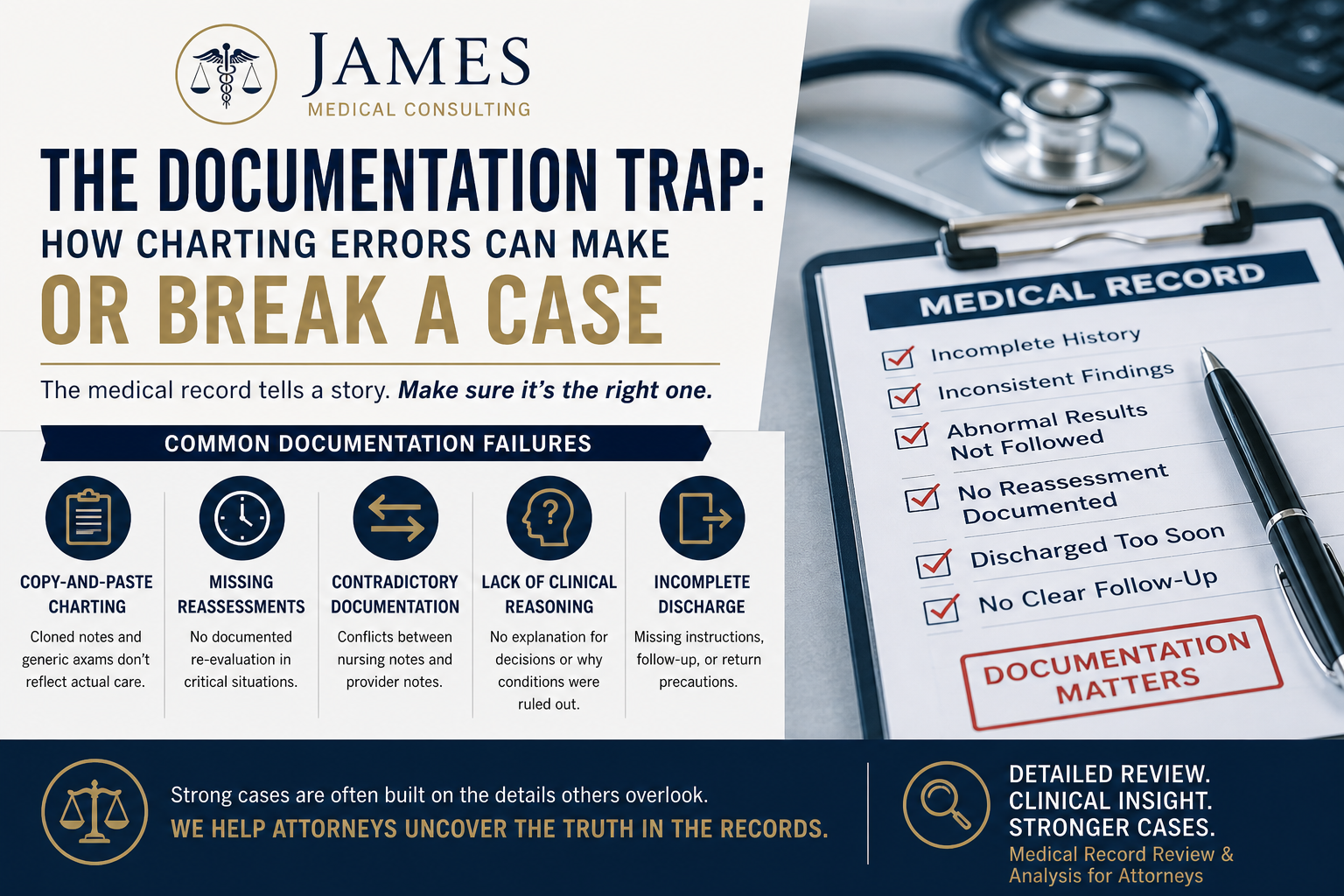
The Documentation Trap: How Charting Errors Can Make or Break a Medical Malpractice Case
Introduction
In medical malpractice cases, the truth is often hidden in plain sight—inside the medical record.
While attorneys often focus on major clinical events, some of the strongest cases are built on something less obvious: documentation errors.
From copy-and-paste notes to missing reassessments, these charting issues can expose deviations from the standard of care, weaken defense arguments, and significantly strengthen causation.
As a Physician Assistant who reviews records for attorneys, I consistently find that documentation tells a deeper story—if you know how to read it.
Why Documentation Matters More Than You Think
Medical records are not just a timeline of care—they are the legal foundation of a case.
When documentation is:
Incomplete
Inconsistent
Or clearly templated
…it raises serious questions about the reliability of the care provided.
In many cases, poor documentation is not just a clerical issue—it reflects poor clinical decision-making.
The Most Common Documentation Failures
1. Copy-and-Paste Charting (“Cloning”)
One of the most frequent issues in modern electronic health records.
What it looks like:
Identical physical exams repeated across multiple visits
“Normal” findings documented despite abnormal vitals or labs
Notes that don’t reflect the patient’s actual condition
Why it matters:
This can undermine credibility and suggest the patient was not properly evaluated.
2. Missing Reassessments
In high-risk scenarios—especially in the emergency department—patients should be reassessed regularly.
Red Flag:
No documented reassessment after treatment or abnormal findings
No updated exam prior to discharge
Legal Impact:
It becomes difficult to justify clinical decisions without evidence the patient was re-evaluated.
3. Contradictory Documentation
Discrepancies between different parts of the chart can be powerful.
Examples:
Nursing notes document severe pain, while provider notes say “patient comfortable”
Vital signs showing instability, but provider documents “stable”
Why this is critical:
These inconsistencies can directly challenge the defense narrative.
4. Lack of Clinical Reasoning
A major issue in many malpractice cases is not what was done—but what wasn’t explained.
What’s missing:
No rationale for ruling out serious conditions
No explanation for not ordering tests
No documentation of differential diagnosis
Impact:
Without documented reasoning, it’s difficult to defend clinical decisions.
5. Incomplete Discharge Documentation
Discharge is one of the highest-risk points in patient care.
Red Flags Include:
No clear diagnosis
No follow-up instructions
No return precautions
Discharge despite abnormal findings
This is a common area where strong cases are built.
How Attorneys Can Spot These Issues Quickly
When reviewing records, look for:
Repeated phrases like “WNL” or “normal exam” across multiple entries
Large gaps in time without documentation
Abnormal results without acknowledgment
Sudden discharge without documented improvement
Conflicts between different providers’ notes
These patterns often point to deeper issues.
Why Early Chart Review Is Critical
The earlier documentation issues are identified, the stronger your case strategy becomes.
Early medical review can:
Clarify whether a case has merit
Identify key deviations from standard of care
Help focus discovery and expert review
Save time and resources
Waiting too long can mean missing critical details that shape the case.
How I Help Attorneys Strengthen Their Cases
Through detailed medical record review, I help attorneys:
Identify documentation inconsistencies and red flags
Break down complex records into clear, actionable insights
Build timelines that highlight gaps in care
Translate medical language into legal strategy
My clinical background allows me to quickly identify the details that matter most.
Conclusion
In medical malpractice cases, documentation is more than just a record—it’s evidence.
And when that evidence is flawed, inconsistent, or incomplete, it can significantly shift the strength of a case.
For attorneys, learning to recognize these patterns can uncover opportunities that might otherwise be missed.

Failure to Follow Up: One of the Most Overlooked Sources of Liability in Medical Malpractice Cases
Introduction
Not every medical error happens at the bedside.
In many malpractice cases, the breakdown occurs after the patient leaves—when abnormal results, critical findings, or necessary follow-up actions fall through the cracks.
Failure to follow up is one of the most overlooked yet highly impactful issues in medical malpractice litigation. And for attorneys, it can be a powerful angle to establish both breach of standard of care and causation.
What Is “Failure to Follow Up”?
Failure to follow up occurs when a healthcare provider or system does not appropriately act on:
Abnormal lab results
Concerning imaging findings
Specialist recommendations
Pending test results at discharge
Necessary outpatient follow-up care
This isn’t always about a missed diagnosis in the moment—it’s about what was known but not acted upon.
Where These Cases Commonly Occur
While this issue can happen in any setting, it is especially common in:
1. Emergency Departments
Patients are often discharged with pending results or incidental findings that require follow-up.
Example:
A CT scan notes a suspicious lesion, but the patient is discharged without notification or referral.
2. Primary Care Settings
Routine labs or imaging may reveal abnormalities that are never communicated or addressed.
Example:
Elevated PSA, abnormal thyroid levels, or concerning blood counts that are not followed up.
3. Hospital Discharges
Transitions of care are a high-risk point.
Red Flags:
No documented follow-up plan
No communication with outpatient providers
Pending results not tracked
Why This Matters Legally
Failure to follow up can significantly strengthen a malpractice case because it often involves:
Clear Documentation
Unlike many clinical decisions, abnormal results are frequently documented and time-stamped.
Missed Opportunity for Intervention
There is often a clear window where action could have changed the outcome.
Strong Causation Arguments
Attorneys can demonstrate:
What was known
What should have been done
How the delay caused harm
Key Red Flags in the Medical Record
When reviewing charts, look for:
Abnormal labs or imaging without documented acknowledgment
Radiology reports with concerning findings and no follow-up plan
Notes that don’t mention previously reported abnormalities
Lack of patient notification documentation
Discharge summaries without clear instructions or referrals
“Pending results” with no tracking or resolution
These details are often where strong cases are built.
The Role of Communication Breakdowns
Many follow-up failures are not due to one provider—but system failures:
Results sent but never reviewed
Messages routed incorrectly in the EHR
Specialists recommending follow-up that is never arranged
Patients not informed of critical findings
Understanding where the breakdown occurred is key to building the case.
Why Early Case Review Is Critical
Failure-to-follow-up cases are highly fact-specific and benefit from early clinical analysis.
Early review can:
Identify whether the standard of care was breached
Establish a clear timeline of missed opportunities
Determine whether earlier intervention would have changed the outcome
Strengthen expert review and legal strategy
How I Help Attorneys Identify These Issues
Through detailed chart review and clinical analysis, I help attorneys:
Identify missed follow-up opportunities
Track abnormal findings across the timeline of care
Highlight documentation gaps and communication failures
Translate complex medical data into clear, actionable insights
This helps build stronger, more focused cases from the start.
Conclusion
Failure to follow up is rarely dramatic—but it is often decisive.
These cases aren’t about what providers didn’t know.
They’re about what they knew—and failed to act on.
For attorneys, recognizing these patterns can uncover powerful opportunities within the medical record.
Missed Diagnosis in the Emergency Department: Where Medical Malpractice Cases Are Won or Lost
Emergency departments are fast-paced, high-pressure environments where providers must make rapid decisions often with limited information. While most care is appropriate, missed or delayed diagnoses remain one of the leading causes of medical malpractice claims.
For attorneys handling personal injury and medical malpractice cases, understanding how and why these diagnostic failures occur can be the difference between a weak claim and a highly defensible case.
As a Physician Assistant with real-world experience reviewing medical records, I consistently see patterns that point to preventable errors—and overlooked opportunities.
Why Missed Diagnoses Happen
Emergency medicine is inherently complex, but certain breakdowns appear repeatedly in malpractice cases:
1. Anchoring Bias
Providers may fixate on an initial diagnosis and fail to adjust when new information becomes available.
Example:
A patient presents with chest pain and is diagnosed with anxiety—despite abnormal vital signs and risk factors for cardiac disease.
2. Inadequate History & Physical Exam
Incomplete documentation or failure to fully assess the patient can lead to critical missed clues.
Red Flag for Attorneys:
Generic documentation such as “normal exam” without detail in high-risk complaints (e.g., abdominal pain, headache, chest pain).
3. Failure to Order Appropriate Diagnostics
Not ordering imaging, labs, or specialty consults when clinically indicated is a common issue.
Common Misses Include:
CT scans for suspected stroke or head bleed
Cardiac workups for chest pain
Imaging for persistent abdominal pain
4. Unfollowed Test Results
One of the most overlooked—and powerful—issues in malpractice cases.
Example:
A radiology report notes a suspicious mass or abnormality, but there is no documentation that the patient was informed or that follow-up was arranged.
This alone can significantly strengthen causation and damages.
5. Premature Discharge
Patients are sometimes discharged before a full evaluation is completed or before their condition stabilizes.
What to Look For:
Minimal observation time
Persistent abnormal vital signs at discharge
No clear discharge instructions or return precautions
Key Medical Record Clues Attorneys Should Look For
When reviewing emergency department records, these details can quickly identify potential negligence:
Time gaps in documentation during critical periods
Copy-and-paste charting (“WNL” repeated across visits)
Contradictions between nursing notes and provider documentation
Abnormal findings without follow-up
Lack of reassessments prior to discharge
These subtle details are often where strong cases are built.
Why Medical Insight Matters Early
One of the biggest mistakes in malpractice litigation is waiting too long to involve a medical consultant.
Early case review can:
Identify deviations from the standard of care
Strengthen case strategy from the start
Save time and resources on weak claims
Highlight documentation inconsistencies that may otherwise be missed
How I Help Attorneys Build Stronger Cases
Through detailed chart review and clinical analysis, I help attorneys:
Break down complex medical records into clear, actionable insights
Identify missed diagnoses and delays in care
Highlight documentation gaps and inconsistencies
Provide timelines that clarify what happened—and what should have happened
My background in emergency and urgent care medicine allows me to quickly identify the issues that matter most.
Conclusion
Missed diagnoses in the emergency department are rarely the result of a single mistake. Instead, they are often the culmination of small oversights, rushed decisions, and documentation failures.
For attorneys, knowing where to look—and what to look for—can transform a case.
If you’re handling a potential malpractice claim and want a clinical perspective early in the process, having the right medical insight can make all the difference.
5 Medical Red Flags Attorneys Often Miss in Med-Mal Cases (And How a PA Expert Can Help) Meta Description
Discover 5 common medical red flags in med-mal cases that attorneys frequently overlook. Matthew James, PA-C, MPH shares clinical insights from real chart reviews to strengthen your cases.
As a practicing Physician Assistant with a Master’s in Public Health and extensive medical-legal consulting experience, I review complex charts for attorneys across plaintiff and defense cases. Electronic health records (EHRs) are dense, and what looks routine on the surface can reveal critical breaches in the standard of care.
Attorneys excel at the legal strategy but clinical nuances often hide in plain sight. Missing these red flags can weaken causation arguments, reduce settlement value, or create vulnerabilities at trial.
Here are five of the most common medical red flags I encounter in med-mal reviews:
1. Incomplete or Inconsistent Vital Signs & Pain Assessments
“Vitals stable” or “WNL” (within normal limits) copied forward without fresh data is a classic issue. Look for gaps in serial monitoring during high-risk periods — post-operative, emergency department visits, or suspected sepsis cases. Pain scores that don’t align with treatment (or are never reassessed) often signal inadequate monitoring of a deteriorating patient. These documentation failures make it harder to prove timely intervention was possible.
2. Unfollowed Abnormal Diagnostic Results
Radiologists or lab reports flag incidental findings (e.g., nodules, abnormal labs, EKG changes), but the ordering provider never follows up or documents patient discussion. This “incidental finding trap” frequently leads to delayed diagnoses in cancer, aneurysms, or infections. Attorneys focusing only on the primary complaint can miss how these overlooked results contributed to harm.
3. Medication Reconciliation & Allergy/Interaction Oversights
EHR systems auto-populate, but errors slip through: outdated allergy lists, continued prescriptions despite known interactions, or “patient denies allergies” contradicted by prior notes. These lead to preventable adverse events like anaphylaxis, bleeding, or acute kidney injury. They’re high-damage but require clinical eyes to connect clearly in the record.
4. Breakdowns in Handoffs or Discharge Instructions
Shift changes, facility transfers, or hospital-to-home discharges often lose critical information. Red flags include absent reconciliation of pending tests, conflicting instructions, or no clear follow-up plan. Communication failures rank among the top root causes in medical errors and are frequently buried in nursing notes or audit trails.
5. Scope-of-Practice or Supervision Issues
Especially relevant in cases involving PAs, NPs, or residents: care provided without required physician oversight, missing co-signatures, or delayed escalations. Louisiana regulations (and similar rules elsewhere) set clear boundaries — violations strengthen vicarious liability and standard-of-care claims.
Why These Red Flags Matter and How I Can Help
Non-clinicians can spend hours in thousands of pages of EHR data and still miss context. A targeted review by a practicing PA creates clean chronologies, identifies breaches, and delivers defensible expert opinions.
I help attorneys:
• Build stronger causation and damages arguments
• Prepare for depositions and trial
• Evaluate case merit early (saving time and resources)
Whether plaintiff or defense, my dual clinical and public health perspective adds unique value to med-mal, personal injury, and healthcare liability matters.
Ready to strengthen your next case?
Contact me today for a fast, thorough medical record review or consultation. Mention this article and I’ll include a complimentary initial case screening summary.
Matthew James, PA-C, MPH
Medical-Legal Consultant
jamesmedicalconsulting@gmail.com
Serving attorneys nationwide with prompt, evidence-based chart reviews and expert support.